
Each year, up to one-quarter of U.S. adults experience low-back pain. Most people have significant back pain at least once in their lives; often, the cause is unknown. Back pain varies widely. For many people, it lasts only a few weeks, no matter what treatment is used. But for others, the pain can become chronic and even debilitating. Low-back pain is a challenging condition to diagnose, treat, and study.
3 Pain Categories
The 3 Main Categories of Pain — each can be mild, moderate, or severe:
1) Acute Pain: Occurs immediately after an injury and lasts no longer than 2 months when treated properly.
2) Chronic Pain: Any type of pain that lasts 6 months or longer. Chronic pain is often difficult to treat, because the cause can be hard to determine. It can also vary from one person to the next — individuals with seemingly the same kind of chronic pain may need different treatments.
3) Cancer Pain: Cancer pain can come from the primary cancer itself (where the cancer started) or from other areas in the body where the cancer has spread by putting pressure on nerves, bones or organs, causing pain.
Scans to Diagnose Chronic Pain Sources:
1) Computed Tomography (CT) Scan
2) Magnetic Resonance Imaging (MRI)
3) Positron Emission Tomography (PET) Scan
Chronic Pain Management
Chronic Pain Management
The treatment option that will work best for you depends on your type of pain, how severe it is, and how you respond to pain treatment. The fact is, only a physician can determine if you are a good candidate for various pain treatment options. Pain Management Specialists are physicians who specialize in treating chronic pain. These physicians receive years of advanced, specialized training in pain management and focus on treating patients with severe pain.
There are 3 Levels of Pain, and each may have different forms of treatment. Usually, your physician will follow a treatment plan that begins with basic therapies (like resting and nutrition) and progresses to more aggressive solutions, depending on the type and severity of pain. The treatment plan also depends on how you respond to any particular treatment.
1) Basic Pain Treatments
- Rest and diet changes
- Exercise and physical therapy
- Anti-inflammatory drugs (ex: ibuprofen)
- Cognitive and behavioral modification
2) Mid-Level Pain Treatments
- Transcutaneous electrical nerve stimulation (TENS)
- Opioids (Prescription painkillers)
- Nerve blocks (injection of an anesthetic, steroid, and/or anti-inflammatory into the pain area)
- Thermal procedures (extreme heat or cold delivered through needles or probes)
3) Advanced Pain Treatments
- Spinal Cord Stimulation (SCS)
SCS, also known as nerve stimulation, uses electrical signals to mask the perception of pain traveling from the painful area to the brain. In place of pain, patients feel a mild tingling sensation called “paresthesia.” SCS may provide long-lasting pain relief and can be used with other therapies. Patients are able to control the intensity of the therapy, as well as turn it on and off, using a wireless remote control. Learn more » - Surgery
Surgical treatments may range from minor outpatient procedures to brain and spinal procedures. Surgery may be needed when structural problems occur within the spinal column often caused by injury or disease. - Implantable Drug Pumps
Pumps deliver pain medication directly to the space surrounding the spinal cord. Direct application reduces the amount of opioids needed to relieve painful symptoms. - Neuroablation
Often used as a last resort when other therapies fail, Neuroablation is a surgical technique that destroys nerves and tissue, permanently blocking nerve signals to the brain.
Back Pain – Overview
What Is Back Pain?
What Is Back Pain?
Back pain is an all-too-familiar problem that can range from a dull, constant ache to a sudden, sharp pain that leaves you incapacitated. It can come on suddenly—from an accident, a fall, or lifting something heavy—or it can develop slowly, perhaps as the result of age-related changes to the spine. Regardless of how back pain happens or how it feels, you know it when you have it. And chances are, if you don’t have back pain now, you will eventually.
How Common Is Back Pain?
In a 3-month period, about one-fourth of U.S. adults experience at least 1 day of back pain. It is one of our society’s most common medical problems.
What Are the Risk Factors for Back Pain?
What Are the Risk Factors for Back Pain?
Although anyone can have back pain, a number of factors increase your risk. They include:
Age: The first attack of low back pain typically occurs between the ages of 30 and 40. Back pain becomes more common with age.
Fitness level: Back pain is more common among people who are not physically fit. Weak back and abdominal muscles may not properly support the spine.


People who go out and exercise a lot after being inactive all week are more likely to suffer painful back injuries than people who make moderate physical activity a daily habit. Studies show that low-impact aerobic exercise is good for the disks that cushion the vertebrae, the individual bones that make up the spine.
Diet: A diet high in calories and fat, combined with an inactive lifestyle, can lead to obesity, which can put stress on the back.
Heredity: Some causes of back pain, such as ankylosing spondylitis, a form of arthritis that affects the spine, have a genetic component.
Race: Race can be a factor in back problems. African American women, for example, are two to three times more likely than white women to develop spondylolisthesis, a condition in which a vertebra of the lower spine—also called the lumbar spine—slips out of place.
The presence of other diseases: Many diseases can cause or contribute to back pain. These include various forms of arthritis, such as osteoarthritis and rheumatoid arthritis, and cancers elsewhere in the body that may spread to the spine.
Occupational risk factors: Having a job that requires heavy lifting, pushing, or pulling, particularly when this involves twisting or vibrating the spine, can lead to injury and back pain. An inactive job or a desk job may also lead to or contribute to pain, especially if you have poor posture or sit all day in an uncomfortable chair.
Cigarette smoking: Although smoking may not directly cause back pain, it increases your risk of developing low back pain and low back pain with sciatica. (Sciatica is back pain that radiates to the hip and/or leg due to pressure on a nerve.) Furthermore, smoking can slow healing, prolonging pain for people who have had back injuries, back surgery, or broken bones.
What Are the Causes of Back Pain?
What Are the Causes of Back Pain?
It is important to understand that back pain is a symptom of a medical condition, not a diagnosis itself. Medical problems that can cause back pain include the following:
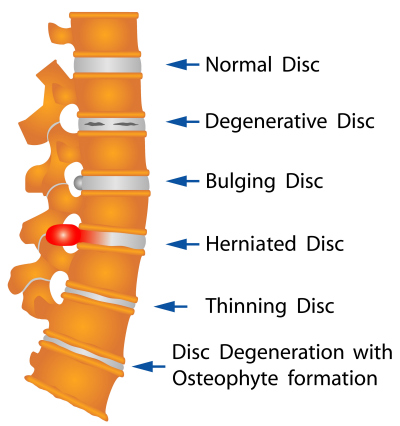
Mechanical problems: A mechanical problem is a problem with the way your spine moves or the way you feel when you move your spine in certain ways. Perhaps the most common mechanical cause of back pain is a condition called intervertebral disk degeneration, which simply means that the disks located between the vertebrae of the spine are breaking down with age. As they deteriorate, they lose their cushioning ability. This problem can lead to pain if the back is stressed. Other mechanical causes of back pain include spasms, muscle tension, and ruptured disks, which are also called herniated disks.
Injuries: Spine injuries such as sprains and fractures can cause either short-lived or chronic pain. Sprains are tears in the ligaments that support the spine, and they can occur from twisting or lifting improperly. Fractured vertebrae are often the result of osteoporosis. Less commonly, back pain may be caused by more severe injuries that result from accidents or falls.
Acquired conditions and diseases: Many medical problems can cause or contribute to back pain. They include scoliosis, a curvature of the spine that does not usually cause pain until middle age; spondylolisthesis; various forms of arthritis, including osteoarthritis, rheumatoid arthritis, and ankylosing spondylitis; and spinal stenosis, a narrowing of the spinal column that puts pressure on the spinal cord and nerves. Although osteoporosis itself is not painful, it can lead to painful fractures of the vertebrae. Other causes of back pain include pregnancy; kidney stones or infections; endometriosis, which is the buildup of uterine tissue in places outside the uterus; and fibromyalgia, a condition of widespread muscle pain and fatigue.
Infections and tumors: Although they are not common causes of back pain, infections can cause pain when they involve the vertebrae, a condition called osteomyelitis, or when they involve the disks that cushion the vertebrae, which is called diskitis. Tumors also are relatively rare causes of back pain. Occasionally, tumors begin in the back, but more often they appear in the back as a result of cancer that has spread from elsewhere in the body.
Although the causes of back pain are usually physical, emotional stress can play a role in how severe pain is and how long it lasts. Stress can affect the body in many ways, including causing back muscles to become tense and painful.
Can Back Pain Be Prevented?
Can Back Pain Be Prevented?
One of the best things you can do to prevent back pain is to exercise regularly and keep your back muscles strong. Four specific types of exercises are described in the section “How Is Back Pain Treated?.” All may help you avoid injury and pain. Exercises that increase balance and strength can decrease your risk of falling and injuring your back or breaking bones. Exercises such as tai chi and yoga—or any weight-bearing exercise that challenges your balance—are good ones to try.
Eating a healthy diet also is important. For one thing, eating to maintain a healthy weight—or to lose weight, if you are overweight—helps you avoid putting unnecessary and injury-causing stress and strain on your back. To keep your spine strong, as with all bones, you need to get enough calcium and vitamin D every day. These nutrients help prevent osteoporosis, which is responsible for a lot of the bone fractures that lead to back pain. Calcium is found in dairy products; green, leafy vegetables; and fortified products, like orange juice. Your skin makes vitamin D when you are in the sun. If you are not outside much, you can obtain vitamin D from your diet: nearly all milk and some other foods are fortified with this nutrient. Most adults don’t get enough calcium and vitamin D, so talk to your doctor about how much you need per day, and consider taking a nutritional supplement or a multivitamin.
Practicing good posture, supporting your back properly, and avoiding heavy lifting when you can may all help you prevent injury. If you do lift something heavy, keep your back straight. Don’t bend over the item; instead, lift it by putting the stress on your legs and hips.
When Should I See a Doctor for Pain?
When Should I See a Doctor for Pain?
In most cases, it is not necessary to see a doctor for back pain because pain usually goes away with or without treatment. However, a trip to the doctor is probably a good idea if you have numbness or tingling, if your pain is severe and doesn’t improve with medication and rest, or if you have pain after a fall or an injury. It is also important to see your doctor if you have pain along with any of the following problems: trouble urinating; weakness, pain, or numbness in your legs; fever; or unintentional weight loss. Such symptoms could signal a serious problem that requires treatment soon.
Which Type of Doctor Should I See?
Many different types of doctors treat back pain, from family physicians to doctors who specialize in disorders of the nerves and musculoskeletal system. In most cases, it is best to see your primary care doctor first. In many cases, he or she can treat the problem. In other cases, your doctor may refer you to an appropriate specialist.
How Is Back Pain Diagnosed?
How Is Back Pain Diagnosed?
Diagnosing the cause of back pain requires a medical history and a physical exam. If necessary, your doctor may also order medical tests, which may include x rays.
During the medical history, your doctor will ask questions about the nature of your pain and about any health problems you and close family members have or have had. Questions might include the following:
- Have you fallen or injured your back recently?
- Does your back feel better—or hurt worse—when you lie down?
- Are there any activities or positions that ease or aggravate pain?
- Is your pain worse or better at a certain time of day?
- Do you or any family members have arthritis or other diseases that might affect the spine?
- Have you had back surgery or back pain before?
- Do you have pain, numbness, or tingling down one or both legs?
During the physical exam, your doctor may:
- watch you stand and walk
- check your reflexes to look for slowed or heightened reflexes, either of which might suggest nerve problems
- check for fibromyalgia by examining your back for tender points, which are points on the body that are painful when pressure is applied to them
- check for muscle strength and sensation
- check for signs of nerve root irritation.
Often a doctor can find the cause of your pain with a physical and medical history alone. However, depending on what the history and exam show, your doctor may order medical tests to help find the cause.
Following are some tests your doctor may order:
X rays: Traditional x rays use low levels of radiation to project a picture onto a piece of film (some newer x rays use electronic imaging techniques). They are often used to view the bones and bony structures in the body. Your doctor may order an x ray if he or she suspects that you have a fracture or osteoarthritis or that your spine is not aligned properly.
Magnetic resonance imaging (MRI): MRI uses a strong magnetic force instead of radiation to create an image. Unlike an x ray, which shows only bony structures, an MRI scan produces clear pictures of soft tissues, too, such as ligaments, tendons, and blood vessels. Your doctor may order an MRI scan if he or she suspects a problem such as an infection, tumor, inflammation, or pressure on a nerve. An MRI scan, in most instances, is not necessary during the early phases of low back pain unless your doctor identifies certain “red flags” in your history and physical exam. An MRI scan is needed if the pain persists for longer than 3 to 6 weeks or if your doctor feels there may be a need for surgical consultation. Because most low back pain goes away on its own, getting an MRI scan too early may sometimes create confusion for the patient and the doctor.
Computed tomography (CT) scan: A CT scan allows your doctor to see spinal structures that cannot be seen on traditional x rays. A computer creates a three-dimensional image from a series of two-dimensional pictures that it takes of your back. Your doctor may order a CT scan to look for problems including herniated disks, tumors, or spinal stenosis.
Blood tests: Although blood tests are not used generally in diagnosing the cause of back pain, your doctor may order them in some cases. Blood tests that might be used include the following:
- Complete blood count (CBC), which could point to problems such as infection or inflammation
- Erythrocyte sedimentation rate (also called sed rate), a measure of inflammation that may suggest infection. The presence of inflammation may also suggest some forms of arthritis or, in rare cases, a tumor.
- C-reactive protein (CRP), another blood test that is used to measure inflammation, may indicate an infection or some forms of arthritis.
- HLA-B27, a test to identify a genetic marker in the blood that is more common in people with ankylosing spondylitis (a form of arthritis that affects the spine and sacroiliac joints) or reactive arthritis (a form of arthritis that occurs following infection in another part of the body, usually the genitourinary tract).
It is important to understand that medical tests alone may not diagnose the cause of back pain. Often, MRI scans of the spine show some type of abnormality, even in people without symptoms. Similarly, even some healthy pain-free people can have elevated sed rates.
Only with a medical history and exam—and sometimes medical tests—can a doctor diagnose the cause of back pain. Many times, the precise cause of back pain is never known. In these cases, it may be comforting to know that most back pain gets better whether or not you find out what is causing it.
What Is the Difference Between Acute and Chronic Pain?
What Is the Difference Between Acute and Chronic Pain?
Pain that hits you suddenly—after falling from a ladder, being tackled on the football field, or lifting a load that is too heavy, for example—is acute pain. Acute pain comes on quickly and often leaves just as quickly. To be classified as acute, pain should last no longer than 6 weeks. Acute pain is the most common type of back pain.
Chronic pain, on the other hand, may come on either quickly or slowly, and it lingers a long time. In general, pain that lasts longer than 3 months is considered chronic. Chronic pain is much less common than acute pain.
How Is Back Pain Treated?
How Is Back Pain Treated?
Treatment for back pain generally depends on what kind of pain you experience: acute or chronic.
Acute Back Pain
Acute back pain usually gets better on its own and without treatment, although you may want to try acetaminophen, aspirin, or ibuprofen to help ease the pain. Perhaps the best advice is to go about your usual activities as much as you can with the assurance that the problem will clear up. Getting up and moving around can help ease stiffness, relieve pain, and have you back doing your regular activities sooner. Exercises or surgery are not usually advisable for acute back pain.
Chronic Back Pain
Treatment for chronic back pain falls into two basic categories: the kind that requires an operation and the kind that does not. In the vast majority of cases, back pain does not require surgery. Doctors will nearly always try nonsurgical treatments before recommending surgery. In a very small percentage of cases—when back pain is caused by a tumor, an infection, or a nerve root problem called cauda equina syndrome, for example—prompt surgery is necessary to ease the pain and prevent further problems.
Following are some of the more commonly used treatments for chronic back pain.
Nonsurgical Treatments
Hot or cold: Hot or cold packs—or sometimes a combination of the two—can be soothing to chronically sore, stiff backs. Heat dilates the blood vessels, both improving the supply of oxygen that the blood takes to the back and reducing muscle spasms. Heat also alters the sensation of pain. Cold may reduce inflammation by decreasing the size of blood vessels and the flow of blood to the area. Although cold may feel painful against the skin, it numbs deep pain. Applying heat or cold may relieve pain, but it does not cure the cause of chronic back pain.
Exercise: Although exercise is usually not advisable for acute back pain, proper exercise can help ease chronic pain and perhaps reduce the risk of it returning. The following four types of exercise are important to general physical fitness and may be helpful for certain specific causes of back pain:
- Flexion: The purposes of flexion exercises, which are exercises in which you bend forward, are to (1) widen the spaces between the vertebrae, thereby reducing pressure on the nerves; (2) stretch muscles of the back and hips; and (3) strengthen abdominal and buttock muscles. Many doctors think that strengthening the muscles of the abdomen will reduce the load on the spine. One word of caution: If your back pain is caused by a herniated disk, check with your doctor before performing flexion exercises because they may increase pressure within the disk, making the problem worse.
- Extension: With extension exercises, you bend backward. They may minimize radiating pain, which is pain you can feel in other parts of the body besides where it originates. Examples of extension exercises are leg lifting and raising the trunk, each exercise performed while lying prone. The theory behind these exercises is that they open up the spinal canal in places and develop muscles that support the spine.
- Stretching: The goal of stretching exercises, as their name suggests, is to stretch and improve the extension of muscles and other soft tissues of the back. This can reduce back stiffness and improve range of motion.
- Aerobic: Aerobic exercise is the type that gets your heart pumping faster and keeps your heart rate elevated for a while. For fitness, it is important to get at least 30 minutes of aerobic (also called cardiovascular) exercise three times a week. Aerobic exercises work the large muscles of the body and include brisk walking, jogging, and swimming. For back problems, you should avoid exercise that requires twisting or vigorous forward flexion, such as aerobic dancing and rowing, because these actions may raise pressure in the disks and actually do more harm than good. In addition, avoid high-impact activities if you have disk disease. If back pain or your fitness level makes it impossible to exercise 30 minutes at a time, try three 10-minute sessions to start with and work up to your goal. But first, speak with your doctor or physical therapist about the safest aerobic exercise for you.
Medications: A wide range of medications are used to treat chronic back pain. Some are available over the counter. Others require a doctor’s prescription. The following are the main types of medications used for back pain.1
1 All medicines can have side effects. Some medicines and side effects are mentioned in this publication. Some side effects may be more severe than others. You should review the package insert that comes with your medicine and ask your health care provider or pharmacist if you have any questions about the possible side effects.
- Analgesics: Analgesic medications are those designed specifically to relieve pain. They include over-thecounter acetaminophen and aspirin, as well as prescription narcotics, such as oxycodone with acetaminophen or hydrocodone with acetaminophen. Aspirin and acetaminophen are the most commonly used analgesics; narcotics should only be used for a short time for severe pain or pain after surgery. People with muscular back pain or arthritis pain that is not relieved by medications may find topical analgesics helpful. These creams, ointments, and salves are rubbed directly onto the skin over the site of pain. They use one or more of a variety of ingredients to ease pain.
- NSAIDs: Nonsteroidal anti-inflammatory drugs (NSAIDs) are drugs that relieve pain and inflammation, both of which may play a role in some cases of back pain. NSAIDs include the nonprescription products ibuprofen, ketoprofen, and naproxen sodium. More than a dozen others, including a subclass of NSAIDs called COX-2 inhibitors, are available only with a prescription.
All NSAIDs work similarly by blocking substances called prostaglandins that contribute to inflammation and pain. However, each NSAID is a different chemical, and each has a slightly different effect on the body.2
2 Warning: Side effects of NSAIDs include stomach problems; skin rashes; high blood pressure; fluid retention; and liver, kidney, and heart problems. The longer a person uses NSAIDs, the more likely he or she is to have side effects, ranging from mild to serious. Many other drugs cannot be taken when a patient is being treated with NSAIDs, because NSAIDs alter the way the body uses or eliminates these other drugs. Check with your health care provider or pharmacist before you take NSAIDs. NSAIDs should only be used at the lowest dose possible for the shortest time needed.
- Side effects of all NSAIDs can include stomach upset and stomach ulcers, heartburn, diarrhea, and fluid retention; however, COX-2 inhibitors are designed to cause fewer stomach ulcers. For unknown reasons, some people seem to respond better to one NSAID than another. It’s important to work with your doctor to choose the one that’s safest and most effective for you.
- Other medications: Muscle relaxants and certain antidepressants have also been prescribed for chronic back pain, but their usefulness is questionable. If the cause of back pain is an inflammatory form of arthritis, medications used to treat that specific form of arthritis may be helpful against the pain.
Traction: Traction involves using pulleys and weights to stretch the back. The rationale behind traction is to pull the vertebrae apart to allow a bulging disk to slip back into place. Some people experience pain relief while in traction, but that relief is usually temporary. Once traction is released, the stretch is not sustained and back pain is likely to return. There is no scientific evidence that traction provides any long-term benefits for people with back pain.
Behavioral modification: Developing a healthy attitude and learning to move your body properly while you do daily activities, particularly those involving heavy lifting, pushing, or pulling, are sometimes part of the treatment plan for people with back pain. Other behavior changes that might help pain include adopting healthy habits, such as exercise, relaxation, and regular sleep, and dropping bad habits, such as smoking and eating poorly.
Injections: When medications and other nonsurgical treatments fail to relieve chronic back pain, doctors may recommend injections for pain relief. Following are some of the most commonly used injections, although some are of questionable value:
- Nerve root blocks: If a nerve is inflamed or compressed as it passes from the spinal column between the vertebrae, an injection called a nerve root block may be used to help ease the resulting back and leg pain. The injection contains a steroid medication or anesthetic and is administered to the affected part of the nerve.
Complementary and alternative treatments: When back pain becomes chronic or when medications and other conventional therapies do not relieve it, many people try complementary and alternative treatments. Although such therapies won’t cure diseases or repair the injuries that cause pain, some people find them useful for managing or relieving pain.
Surgical Treatments
Depending on the diagnosis, surgery may either be the first treatment of choice—although this is rare—or it is reserved for chronic back pain for which other treatments have failed. If you are in constant pain or if pain reoccurs frequently and interferes with your ability to sleep, to function at your job, or to perform daily activities, you may be a candidate for surgery.
In general, two groups of people may require surgery to treat their spinal problems. People in the first group have chronic low back pain and sciatica, and they are often diagnosed with a herniated disk, spinal stenosis, spondylolisthesis, or vertebral fractures with nerve involvement. People in the second group are those with only predominant low back pain (without leg pain). These are people with diskogenic low back pain (degenerative disk disease), in which disks wear with age. Usually, the outcome of spine surgery is much more predictable in people with sciatica than in those with predominant low back pain.
Some of the diagnoses that may need surgery include:
Herniated disks: In this potentially painful problem, the hard outer coating of the disks, which are the circular pieces of connective tissue that cushion the bones of the spine, are damaged, allowing the disks’ jelly-like center to leak, irritating nearby nerves. This causes severe sciatica and nerve pain down the leg. A herniated disk is sometimes called a ruptured disk.
Spinal stenosis: Spinal stenosis is the narrowing of the spinal canal, through which the spinal cord and spinal nerves run. It is often caused by the overgrowth of bone caused by osteoarthritis of the spine. Compression of the nerves caused by spinal stenosis can lead not only to pain, but also to numbness in the legs and the loss of bladder or bowel control. Patients may have difficulty walking any distance and may have severe pain in their legs along with numbness and tingling.
Spondylolisthesis: In this condition, a vertebra of the lumbar spine slips out of place. As the spine tries to stabilize itself, the joints between the slipped vertebra and adjacent vertebrae can become enlarged, pinching nerves as they exit the spinal column. Spondylolisthesis may cause not only low back pain but also severe sciatica leg pain.
Vertebral fractures: These fractures are caused by trauma to the vertebrae of the spine or by crumbling of the vertebrae resulting from osteoporosis. This causes mostly mechanical back pain, but it may also put pressure on the nerves, creating leg pain.
Diskogenic low back pain (degenerative disk disease): Most people’s disks degenerate over a lifetime, but in some, this aging process can become chronically painful, severely interfering with their quality of life.
Following are some of the most commonly performed back surgeries:
For herniated disks:
Laminectomy/diskectomy: In this operation, part of the lamina, a portion of the bone on the back of the vertebrae, is removed, as well as a portion of a ligament. The herniated disk is then removed through the incision, which may extend two or more inches.
Microdiskectomy: As with traditional diskectomy, this procedure involves removing a herniated disk or damaged portion of a disk through an incision in the back. The difference is that the incision is much smaller and the doctor uses a magnifying microscope or lenses to locate the disk through the incision. The smaller incision may reduce pain and the disruption of tissues, and it reduces the size of the surgical scar. It appears to take about the same amount of time to recuperate from a microdiskectomy as from a traditional diskectomy.
Laser surgery: Technological advances in recent decades have led to the use of lasers for operating on patients with herniated disks accompanied by lower back and leg pain. During this procedure, the surgeon inserts a needle in the disk that delivers a few bursts of laser energy to vaporize the tissue in the disk. This reduces its size and relieves pressure on the nerves. Although many patients return to daily activities within 3 to 5 days after laser surgery, pain relief may not be apparent until several weeks or even months after the surgery. The usefulness of laser diskectomy is still being debated.
For spinal stenosis:
Laminectomy: When narrowing of the spine compresses the nerve roots, causing pain or affecting sensation, doctors sometimes open up the spinal column with a procedure called a laminectomy. In a laminectomy, the doctor makes a large incision down the affected area of the spine and removes the lamina and any bone spurs, which are overgrowths of bone that may have formed in the spinal canal as the result of osteoarthritis. The procedure is major surgery that requires a short hospital stay and physical therapy afterwards to help regain strength and mobility.
For spondylolisthesis:
Spinal fusion: When a slipped vertebra leads to the enlargement of adjacent facet joints, surgical treatment generally involves both laminectomy (as described above) and spinal fusion. In spinal fusion, two or more vertebrae are joined together using bone grafts, screws, and rods to stop slippage of the affected vertebrae. Bone used for grafting comes from another area of the body, usually the hip or pelvis. In some cases, donor bone is used.
Although the surgery is generally successful, either type of graft has its drawbacks. Using your own bone means surgery at a second site on your body. With donor bone, there is a slight risk of disease transmission or tissue rejection, which happens when your immune system attacks the donor tissue. In recent years, a new development has eliminated those risks for some people undergoing spinal fusion: proteins called bone morphogenic proteins are being used to stimulate bone generation, eliminating the need for grafts. The proteins are placed in the affected area of the spine, often in collagen putty or sponges.
Regardless of how spinal fusion is performed, the fused area of the spine becomes immobilized.
For vertebral osteoporotic fractures:
Vertebroplasty: When back pain is caused by a compression fracture of a vertebra caused by osteoporosis or trauma, doctors may make a small incision in the skin over the affected area and inject a cement-like mixture called polymethylacrylate into the fractured vertebra to relieve pain and stabilize the spine.3 The procedure is generally performed on an outpatient basis under a mild anesthetic.
3 Used only if standard care, rest, corsets and braces, and analgesics fail.
Kyphoplasty: Much like vertebroplasty, kyphoplasty is used to relieve pain and stabilize the spine following fractures caused by osteoporosis. Kyphoplasty is a twostep process. In the first step, the doctor inserts a balloon device to help restore the height and shape of the spine. In the second step, he or she injects polymethylacrylate to repair the fractured vertebra. The procedure is done under anesthesia, and in some cases it is performed on an outpatient basis.
For diskogenic low back pain (degenerative disk disease):
Intradiskal electrothermal therapy (IDET): One of the least invasive therapies for low back pain involves inserting a heating wire through a small incision in the back and into a disk. An electrical current is then passed through the wire to strengthen the collagen fibers that hold the disk together. The procedure is done on an outpatient basis, often under local anesthesia. The effectiveness of IDET is not clear.
Spinal fusion: When the degenerated disk is painful, the surgeon may recommend removing it and fusing the disk to help with the pain. This fusion can be done through the abdomen, a procedure known as anterior lumbar interbody fusion, or through the back, called posterior fusion. Fusion for low back pain or any spinal surgeries should only be done as a last resort, and the patient should be fully informed of risks.
Disk replacement: When a disk is herniated, one alternative to a diskectomy, in which the disk is simply removed, is removing the disk and replacing it with a synthetic disk. Replacing the damaged one with an artificial one restores disk height and movement between the vertebrae. Artificial disks come in several designs.


Low Back Pain – Details
Low Back Pain
Men and women are equally affected by low back pain, which can range in intensity from a dull, constant ache to a sudden, sharp sensation that leaves the person incapacitated. Pain can begin abruptly as a result of an accident or by lifting something heavy, or it can develop over time due to age-related changes of the spine. Sedentary lifestyles also can set the stage for low back pain, especially when a weekday routine of getting too little exercise is punctuated by strenuous weekend workout.
Most low back pain is acute, or short term, and lasts a few days to a few weeks. It tends to resolve on its own with self-care and there is no residual loss of function. The majority of acute low back pain is mechanical in nature, meaning that there is a disruption in the way the components of the back (the spine, muscle, intervertebral discs, and nerves) fit together and move.
Subacute low back pain is defined as pain that lasts between 4 and 12 weeks.
Chronic back pain is defined as pain that persists for 12 weeks or longer, even after an initial injury or underlying cause of acute low back pain has been treated. About 20 percent of people affected by acute low back pain develop chronic low back pain with persistent symptoms at one year. In some cases, treatment successfully relieves chronic low back pain, but in other cases pain persists despite medical and surgical treatment.
The magnitude of the burden from low back pain has grown worse in recent years. In 1990, a study ranking the most burdensome conditions in the U.S. in terms of mortality or poor health as a result of disease put low back pain in sixth place; in 2010, low back pain jumped to third place, with only ischemic heart disease and chronic obstructive pulmonary disease ranking higher.
What Structures Make Up The Back?
What Structures make up the Back?
The lower back where most back pain occurs includes the five vertebrae (referred to as L1-L5) in the lumbar region, which supports much of the weight of the upper body. The spaces between the vertebrae are maintained by round, rubbery pads called intervertebral discs that act like shock absorbers throughout the spinal column to cushion the bones as the body moves. Bands of tissue known as ligaments hold the vertebrae in place, and tendons attach the muscles to the spinal column. Thirty-one pairs of nerves are rooted to the spinal cord and they control body movements and transmit signals from the body to the brain.
What Causes Lower Back Pain?
What causes Lower Back Pain?
The vast majority of low back pain is mechanical in nature. In many cases, low back pain is associated with spondylosis, a term that refers to the general degeneration of the spine associated with normal wear and tear that occurs in the joints, discs, and bones of the spine as people get older. Some examples of mechanical causes of low back pain include:
- Sprains and Strains account for most acute back pain. Sprains are caused by overstretching or tearing ligaments, and strains are tears in tendon or muscle. Both can occur from twisting or lifting something improperly, lifting something too heavy, or overstretching. Such movements may also trigger spasms in back muscles, which can also be painful.
- Intervertebral Disc Degeneration is one of the most common mechanical causes of low back pain, and it occurs when the usually rubbery discs lose integrity as a normal process of aging. In a healthy back, intervertebral discs provide height and allow bending, flexion, and torsion of the lower back. As the discs deteriorate, they lose their cushioning ability.
- Herniated or Ruptured Discs can occur when the intervertebral discs become compressed and bulge outward (herniation) or rupture, causing low back pain.
- Radiculopathy is a condition caused by compression, inflammation and/or injury to a spinal nerve root. Pressure on the nerve root results in pain, numbness, or a tingling sensation that travels or radiates to other areas of the body that are served by that nerve. Radiculopathy may occur when spinal stenosis or a herniated or ruptured disc compresses the nerve root.
- Sciatica is a form of radiculopathy caused by compression of the sciatic nerve, the large nerve that travels through the buttocks and extends down the back of the leg. This compression causes shock-like or burning low back pain combined with pain through the buttocks and down one leg, occasionally reaching the foot. In the most extreme cases, when the nerve is pinched between the disc and the adjacent bone, the symptoms may involve not only pain, but numbness and muscle weakness in the leg because of interrupted nerve signaling. The condition may also be caused by a tumor or cyst that presses on the sciatic nerve or its roots.
- Spondylolisthesis is a condition in which a vertebra of the lower spine slips out of place, pinching the nerves exiting the spinal column.
- A Traumatic Injury, such as from playing sports, car accidents, or a fall can injure tendons, ligaments or muscle resulting in low back pain. Traumatic injury may also cause the spine to become overly compressed, which in turn can cause an intervertebral disc to rupture or herniate, exerting pressure on any of the nerves rooted to the spinal cord. When spinal nerves become compressed and irritated, back pain and sciatica may result.
- Spinal Stenosis is a narrowing of the spinal column that puts pressure on the spinal cord and nerves that can cause pain or numbness with walking and over time leads to leg weakness and sensory loss.
- Skeletal Irregularities include scoliosis, a curvature of the spine that does not usually cause pain until middle age; lordosis, an abnormally accentuated arch in the lower back; and other congenital anomalies of the spine.
Low back pain is rarely related to serious underlying conditions, but when these conditions do occur, they require immediate medical attention. Serious underlying conditions include:
- Infections are not a common cause of back pain. However, infections can cause pain when they involve the vertebrae, a condition called osteomyelitis; the intervertebral discs, called discitis; or the sacroiliac joints connecting the lower spine to the pelvis, called sacroiliitis.
- Tumors are a relatively rare cause of back pain. Occasionally, tumors begin in the back, but more often they appear in the back as a result of cancer that has spread from elsewhere in the body.
- Cauda Equina Syndrome is a serious but rare complication of a ruptured disc. It occurs when disc material is pushed into the spinal canal and compresses the bundle of lumbar and sacral nerve roots, causing loss of bladder and bowel control. Permanent neurological damage may result if this syndrome is left untreated.
- Abdominal Aortic Aneurysms occur when the large blood vessel that supplies blood to the abdomen, pelvis, and legs becomes abnormally enlarged. Back pain can be a sign that the aneurysm is becoming larger and that the risk of rupture should be assessed.
- Kidney Stones can cause sharp pain in the lower back, usually on one side.
Other underlying conditions that predispose people to low back pain include:
- Inflammatory Diseases of the Joints such as arthritis, including osteoarthritis and rheumatoid arthritis as well as spondylitis, an inflammation of the vertebrae, can also cause low back pain. Spondylitis is also called spondyloarthritis or spondyloarthropathy.
- Osteoporosis is a metabolic bone disease marked by a progressive decrease in bone density and strength, which can lead to painful fractures of the vertebrae.
- Endometriosis is the buildup of uterine tissue in places outside the uterus.
- Fibromyalgia, a chronic pain syndrome involving widespread muscle pain and fatigue.
What are the Risk Factors for Developing Low Back Pain?
What are the risk factors for developing low back pain?
Beyond underlying diseases, certain other risk factors may elevate one’s risk for low back pain, including:
Age: The first attack of low back pain typically occurs between the ages of 30 and 50, and back pain becomes more common with advancing age. As people grow older, loss of bone strength from osteoporosis can lead to fractures, and at the same time, muscle elasticity and tone decrease. The intervertebral discs begin to lose fluid and flexibility with age, which decreases their ability to cushion the vertebrae. The risk of spinal stenosis also increases with age.
Fitness Level: Back pain is more common among people who are not physically fit. Weak back and abdominal muscles may not properly support the spine. “Weekend warriors”—people who go out and exercise a lot after being inactive all week—are more likely to suffer painful back injuries than people who make moderate physical activity a daily habit. Studies show that low-impact aerobic exercise is beneficial for the maintaining the integrity of intervertebral discs.
Pregnancy is commonly accompanied by low back pain, which results from pelvic changes and alterations in weight loading. Back symptoms almost always resolve postpartum.
Weight Gain: Being overweight, obese, or quickly gaining significant amounts of weight can put stress on the back and lead to low back pain.
Genetics: Some causes of back pain, such as ankylosing spondylitis, a form of arthritis that involves fusion of the spinal joints leading to some immobility of the spine, have a genetic component.
Occupational Risk Factors: Having a job that requires heavy lifting, pushing, or pulling, particularly when it involves twisting or vibrating the spine, can lead to injury and back pain. An inactive job or a desk job may also lead to or contribute to pain, especially if you have poor posture or sit all day in a chair with inadequate back support.
Mental Health Factors: Pre-existing mental health issues such as anxiety and depression can influence how closely one focuses on their pain as well as their perception of its severity. Pain that becomes chronic also can contribute to the development of such psychological factors. Stress can affect the body in numerous ways, including causing muscle tension.
Backpack Overload in Children: Low back pain unrelated to injury or other known cause is unusual in pre-teen children. However, a backpack overloaded with schoolbooks and supplies can strain the back and cause muscle fatigue. The American Academy of Orthopaedic Surgeons recommends that a child’s backpack should weigh no more than 15 to 20 percent of the child’s body weight.
How is Low Back Pain Diagnosed?
How is low back pain diagnosed?
A complete medical history and physical exam can usually identify any serious conditions that may be causing the pain. During the exam, a health care provider will ask about the onset, site, and severity of the pain; duration of symptoms and any limitations in movement; and history of previous episodes or any health conditions that might be related to the pain. Along with a thorough back examination, neurologic tests are conducted to determine the cause of pain and appropriate treatment. The cause of chronic lower back pain is often difficult to determine even after a thorough examination.
Imaging tests are not warranted in most cases. Under certain circumstances, however, imaging may be ordered to rule out specific causes of pain, including tumors and spinal stenosis. Imaging and other types of tests include:
X-ray is often the first imaging technique used to look for broken bones or an injured vertebra. X-rays show the bony structures and any vertebral misalignment or fractures. Soft tissues such as muscles, ligaments, or bulging discs are not visible on conventional x-rays.
Computerized Tomography (CT) is used to see spinal structures that cannot be seen on conventional x-rays, such as disc rupture, spinal stenosis, or tumors. Using a computer, the CT scan creates a three-dimensional image from a series of two dimensional pictures.
Myelograms enhance the diagnostic imaging of x-rays and CT scans. In this procedure, a contrast dye is injected into the spinal canal, allowing spinal cord and nerve compression caused by herniated discs or fractures to be seen on an x-ray or CT scans.
Discography may be used when other diagnostic procedures fail to identify the cause of pain. This procedure involves the injection of a contrast dye into a spinal disc thought to be causing low back pain. The fluid’s pressure in the disc will reproduce the person’s symptoms if the disc is the cause. The dye helps to show the damaged areas on CT scans taken following the injection. Discography may provide useful information in cases where people are considering lumbar surgery or when their pain has not responded to conventional treatments.
Magnetic Resonance Imaging (MRI) uses a magnetic force instead of radiation to create a computer-generated image. Unlike x-ray, which shows only bony structures, MRI scans also produce images of soft tissues such as muscles, ligaments, tendons, and blood vessels. An MRI may be ordered if a problem such as infection, tumor, inflammation, disc herniation or rupture, or pressure on a nerve is suspected. MRI is a noninvasive way to identify a condition requiring prompt surgical treatment. However, in most instances, unless there are “red flags” in the history or physical exam, an MRI scan is not necessary during the early phases of low back pain.
Electrodiagnostics are procedures that, in the setting of low back pain, are primarily used to confirm whether a person has lumbar radiculopathy. The procedures include electromyography (EMG), nerve conduction studies (NCS), and evoked potential (EP) studies. EMG assesses the electrical activity in a muscle and can detect if muscle weakness results from a problem with the nerves that control the muscles. Very fine needles are inserted in muscles to measure electrical activity transmitted from the brain or spinal cord to a particular area of the body. NCSs are often performed along with EMG to exclude conditions that can mimic radiculopathy. In NCSs, two sets of electrodes are placed on the skin over the muscles. The first set provides a mild shock to stimulate the nerve that runs to a particular muscle. The second set records the nerve’s electrical signals, and from this information nerve damage that slows conduction of the nerve signal can be detected. EP tests also involve two sets of electrodes—one set to stimulate a sensory nerve, and the other placed on the scalp to record the speed of nerve signal transmissions to the brain.
Bone Scans are used to detect and monitor infection, fracture, or disorders in the bone. A small amount of radioactive material is injected into the bloodstream and will collect in the bones, particularly in areas with some abnormality. Scanner-generated images can be used to identify specific areas of irregular bone metabolism or abnormal blood flow, as well as to measure levels of joint disease.
Ultrasound Imaging, also called ultrasound scanning or sonography, uses high-frequency sound waves to obtain images inside the body. The sound wave echoes are recorded and displayed as a real-time visual image. Ultrasound imaging can show tears in ligaments, muscles, tendons, and other soft tissue masses in the back.
Blood Tests are not routinely used to diagnose the cause of back pain; however in some cases they may be ordered to look for indications of inflammation, infection, and/or the presence of arthritis. Potential tests include complete blood count, erythrocyte sedimentation rate, and C-reactive protein. Blood tests may also detect HLA-B27, a genetic marker in the blood that is more common in people with ankylosing spondylitis or reactive arthritis (a form of arthritis that occurs following infection in another part of the body, usually the genitourinary tract).
How is Back Pain Treated?
How is back pain treated?
Treatment for low back pain generally depends on whether the pain is acute or chronic. In general, surgery is recommended only if there is evidence of worsening nerve damage and when diagnostic tests indicate structural changes for which corrective surgical procedures have been developed.
Conventionally used treatments and their level of supportive evidence include:
Hot or cold packs have never been proven to quickly resolve low back injury; however, they may help ease pain and reduce inflammation for people with acute, subacute, or chronic pain, allowing for greater mobility among some individuals.
Activity: Bed rest should be limited. Individuals should begin stretching exercises and resume normal daily activities as soon as possible, while avoiding movements that aggravate pain. Strong evidence shows that persons who continue their activities without bed rest following onset of low back pain appeared to have better back flexibility than those who rested in bed for a week. Other studies suggest that bed rest alone may make back pain worse and can lead to secondary complications such as depression, decreased muscle tone, and blood clots in the legs.
Strengthening exercises, beyond general daily activities, are not advised for acute low back pain, but may be an effective way to speed recovery from chronic or subacute low back pain. Maintaining and building muscle strength is particularly important for persons with skeletal irregularities. Health care providers can provide a list of beneficial exercises that will help improve coordination and develop proper posture and muscle balance. Evidence supports short- and long-term benefits of yoga to ease chronic low back pain.
Physical therapy programs to strengthen core muscle groups that support the low back, improve mobility and flexibility, and promote proper positioning and posture are often used in combinations with other interventions.
Medications: A wide range of medications are used to treat acute and chronic low back pain. Some are available over the counter (OTC); others require a physician’s prescription. Certain drugs, even those available OTC, may be unsafe during pregnancy, may interact with other medications, cause side effects, or lead to serious adverse effects such as liver damage or gastrointestinal ulcers and bleeding. Consultation with a health care provider is advised before use. The following are the main types of medications used for low back pain:
- Analgesic medications are those specifically designed to relieve pain. They include OTC acetaminophen and aspirin, as well as prescription opioids such as codeine, oxycodone, hydrocodone, and morphine. Opioids should be used only for a short period of time and under a physician’s supervision. People can develop a tolerance to opioids and require increasingly higher dosages to achieve the same effect. Opioids can also be addictive. Their side effects can include drowsiness, constipation, decreased reaction time, and impaired judgment. Some specialists are concerned that chronic use of opioids is detrimental to people with back pain because they can aggravate depression, leading to a worsening of the pain.
- Nonsteroidal anti-inflammatory drugs (NSAIDS) relieve pain and inflammation and include OTC formulations (ibuprofen, ketoprofen, and naproxen sodium). Several others, including a type of NSAID called COX-2 inhibitors, are available only by prescription. Long-term use of NSAIDs has been associated with stomach irritation, ulcers, heartburn, diarrhea, fluid retention, and in rare cases, kidney dysfunction and cardiovascular disease. The longer a person uses NSAIDs the more likely they are to develop side effects. Many other drugs cannot be taken at the same time a person is treated with NSAIDs because they alter the way the body processes or eliminates other medications.
- Anticonvulsants—drugs primarily used to treat seizures—may be useful in treating people with radiculopathy and radicular pain.
- Antidepressants such as tricyclics and serotonin and norepinephrine reuptake inhibitors have been commonly prescribed for chronic low back pain, but their benefit for nonspecific low back pain is unproven, according to a review of studies assessing their benefit.
- Counter-irritants such as creams or sprays applied topically stimulate the nerves in the skin to provide feelings of warmth or cold in order to dull the sensation of pain. Topical analgesics reduce inflammation and stimulate blood flow.
Spinal manipulation and spinal mobilization are approaches in which professionally licensed specialists (doctors of chiropractic care) use their hands to mobilize, adjust, massage, or stimulate the spine and the surrounding tissues. Manipulation involves a rapid movement over which the individual has no control; mobilization involves slower adjustment movements. The techniques have been shown to provide small to moderate short-term benefits in people with chronic low back pain. Evidence supporting their use for acute or subacute low back pain is generally of low quality. Neither technique is appropriate when a person has an underlying medical cause for the back pain such as osteoporosis, spinal cord compression, or arthritis.
Traction involves the use of weights and pulleys to apply constant or intermittent force to gradually “pull” the skeletal structure into better alignment. Some people experience pain relief while in traction, but that relief is usually temporary. Once traction is released the back pain tends to return. There is no evidence that traction provides any longterm benefits for people with low back pain.
Acupuncture is moderately effective for chronic low back pain. It involves the insertion of thin needles into precise points throughout the body. Some practitioners believe this process helps clear away blockages in the body’s life force known as Qi (pronounced chee). Others who may not believe in the concept of Qi theorize that when the needles are inserted and then stimulated (by twisting or passing a low-voltage electrical current through them) naturally occurring painkilling chemicals such as endorphins, serotonin, and acetylcholine are released. Evidence of acupuncture’s benefit for acute low back pain is conflicting and clinical studies continue to investigate its benefits.
Biofeedback is used to treat many acute pain problems, most notably back pain and headache. The therapy involves the attachment of electrodes to the skin and the use of an electromyography machine that allows people to become aware of and selfregulate their breathing, muscle tension, heart rate, and skin temperature. People regulate their response to pain by using relaxation techniques. Biofeedback is often used in combination with other treatment methods, generally without side effects. Evidence is lacking that biofeedback provides a clear benefit for low back pain.
Nerve block therapies aim to relieve chronic pain by blocking nerve conduction from specific areas of the body. Nerve block approaches range from injections of local anesthetics, botulinum toxin, or steroids into affected soft tissues or joints to more complex nerve root blocks and spinal cord stimulation. When extreme pain is involved, low doses of drugs may be administered by catheter directly into the spinal cord. The success of a nerve block approach depends on the ability of a practitioner to locate and inject precisely the correct nerve. Chronic use of steroid injections may lead to increased functional impairment.
Epidural steroid injections are a commonly used short-term option for treating low back pain and sciatica associated with inflammation. Pain relief associated with the injections, however, tends to be temporary and the injections are not advised for long-term use. An NIH-funded randomized controlled trial assessing the benefit of epidural steroid injections for the treatment of chronic low back pain associated with spinal stenosis showed that long-term outcomes were worse among those people who received the injections compared with those who did not.
Transcutaneous electrical nerve stimulation (TENS) involves wearing a battery-powered device consisting of electrodes placed on the skin over the painful area that generate electrical impulses designed to block incoming pain signals from the peripheral nerves. The theory is that stimulating the nervous system can modify the perception of pain. Early studies of TENS suggested that it elevated levels of endorphins, the body’s natural pain-numbing chemicals. More recent studies, however, have produced mixed results on its effectiveness for providing relief from low back pain.
Surgery
When other therapies fail, surgery may be considered an option to relieve pain caused by serious musculoskeletal injuries or nerve compression. It may be months following surgery before the patient is fully healed, and he or she may suffer permanent loss of flexibility.
Surgical procedures are not always successful, and there is little evidence to show which procedures work best for their particular indications. Patients considering surgical approaches should be fully informed of all related risks. Surgical options include:
- Vertebroplasty and kyphoplasty are minimally invasive treatments to repair compression fractures of the vertebrae caused by osteoporosis. Vertebroplasty uses three-dimensional imaging to assist in guiding a fine needle through the skin into the vertebral body, the largest part of the vertebrae. A glue-like bone cement is then injected into the vertebral body space, which quickly hardens to stabilize and strengthen the bone and provide pain relief. In kyphoplasty, prior to injecting the bone cement, a special balloon is inserted and gently inflated to restore height to the vertebral structure and reduce spinal deformity.
- Spinal laminectomy (also known as spinal decompression) is performed when spinal stenosis causes a narrowing of the spinal canal that causes pain, numbness, or weakness. During the procedure, the lamina or bony walls of the vertebrae, along with any bone spurs, are removed. The aim of the procedure is to open up the spinal column to remove pressure on the nerves.
- Discectomy or microdiscectomy may be recommended to remove a disc, in cases where it has herniated and presses on a nerve root or the spinal cord, which may cause intense and enduring pain. Microdiscectomy is similar to a conventional discectomy; however, this procedure involves removing the herniated disc through a much smaller incision in the back and a more rapid recovery. Laminectomy and discectomy are frequently performed together and the combination is one of the more common ways to remove pressure on a nerve root from a herniated disc or bone spur.
- Foraminotomy is an operation that “cleans out” or enlarges the bony hole (foramen) where a nerve root exits the spinal canal. Bulging discs or joints thickened with age can cause narrowing of the space through which the spinal nerve exits and can press on the nerve, resulting in pain, numbness, and weakness in an arm or leg. Small pieces of bone over the nerve are removed through a small slit, allowing the surgeon to cut away the blockage and relieve pressure on the nerve.
- Intradiscal electrothermal therapy (IDET) is a treatment for discs that are cracked or bulging as a result of degenerative disc disease. The procedure involves inserting a catheter through a small incision at the site of the disc in the back. A special wire is passed through the catheter and an electrical current is applied to heat the disc, which helps strengthen the collagen fibers of the disc wall, reducing the bulging and the related irritation of the spinal nerve. IDET is of questionable benefit.
- Nucleoplasty, also called plasma disc decompression (PDD), is a type of laser surgery that uses radiofrequency energy to treat people with low back pain associated with mildly herniated discs. Under x-ray guidance, a needle is inserted into the disc. A plasma laser device is then inserted into the needle and the tip is heated to 40-70 degrees Celsius, creating a field that vaporizes the tissue in the disc, reducing its size and relieving pressure on the nerves. Several channels may be made depending on how tissue needs to be removed to decompress the disc and nerve root.Radiofrequency denervation is a procedure using electrical impulses to interrupt nerve conduction (including the conduction of pain signals). Using x-ray guidance, a needle is inserted into a target area of nerves and a local anesthetic is introduced as a way of confirming the involvement of the nerves in the person’s back pain. Next, the region is heated, resulting in localized destruction of the target nerves. Pain relief associated with the technique is temporary and the evidence supporting this technique is limited.
- Spinal fusion is used to strengthen the spine and prevent painful movements in people with degenerative disc disease or spondylolisthesis (following laminectomy). The spinal disc between two or more vertebrae is removed and the adjacent vertebrae are “fused” by bone grafts and/or metal devices secured by screws. The fusion can be performed through the abdomen, a procedure known as an anterior lumbar interbody fusion, or through the back, called posterior fusion. Spinal fusion may result in some loss of flexibility in the spine and requires a long recovery period to allow the bone grafts to grow and fuse the vertebrae together. Spinal fusion has been associated with an acceleration of disc degeneration at adjacent levels of the spine.
- Artificial disc replacement is considered an alternative to spinal fusion for the treatment of people with severely damaged discs. The procedure involves removal of the disc and its replacement by a synthetic disc that helps restore height and movement between the vertebrae.
Can Back Pain Be Prevented?
Can back pain be prevented?
Recurring back pain resulting from improper body mechanics is often preventable by avoiding movements that jolt or strain the back, maintaining correct posture, and lifting objects properly. Many work-related injuries are caused or aggravated by stressors such as heavy lifting, contact stress (repeated or constant contact between soft body tissue and a hard or sharp object), vibration, repetitive motion, and awkward posture. Using ergonomically designed furniture and equipment to protect the body from injury at home and in the workplace may reduce the risk of back injury.
The use of lumbar supports in the form of wide elastic bands that can be tightened to provide support to the lower back and abdominal muscles to prevent low back pain remains controversial. Such supports are widely used despite a lack of evidence showing that they actually prevent pain. Multiple studies have determined that the use of lumbar supports provides no benefit in terms of the prevention and treatment of back pain. Although there have been anecdotal case reports of injury reduction among workers using lumbar support belts, many companies that have back belt programs also have training and ergonomic awareness programs. The reported injury reduction may be related to a combination of these or other factors. Furthermore, some caution is advised given that wearing supportive belts may actually lead to or aggravate back pain by causing back muscles to weaken from lack of use.
Recommendations For Keeping One's Back Healthy
Recommendations for eeping One’s Back Healthy
Following any period of prolonged inactivity, a regimen of low-impact exercises is advised. Speed walking, swimming, or stationary bike riding 30 minutes daily can increase muscle strength and flexibility. Yoga also can help stretch and strengthen muscles and improve posture. Consult a physician for a list of low-impact, age-appropriate exercises that are specifically targeted to strengthening lower back and abdominal muscles.
- Always stretch before exercise or other strenuous physical activity.
- Don’t slouch when standing or sitting. The lower back can support a person’s weight most easily when the curvature is reduced. When standing, keep your weight balanced on your feet.
- At home or work, make sure work surfaces are at a comfortable height.
- Sit in a chair with good lumbar support and proper position and height for the task. Keep shoulders back. Switch sitting positions often and periodically walk around the office or gently stretch muscles to relieve tension. A pillow or rolled-up towel placed behind the small of the back can provide some lumbar support. During prolonged periods of sitting, elevate feet on a low stool or a stack of books.
- Wear comfortable, low-heeled shoes.
- Sleeping on one’s side with the knees drawn up in a fetal position can help open up the joints in the spine and relieve pressure by reducing the curvature of the spine. Always sleep on a firm surface.
- Don’t try to lift objects that are too heavy. Lift from the knees, pull the stomach muscles in, and keep the head down and in line with a straight back. When lifting, keep objects close to the body. Do not twist when lifting.
- Maintain proper nutrition and diet to reduce and prevent excessive weight gain, especially weight around the waistline that taxes lower back muscles. A diet with sufficient daily intake of calcium, phosphorus, and vitamin D helps to promote new bone growth.
- Quit smoking. Smoking reduces blood flow to the lower spine, which can contribute to spinal disc degeneration. Smoking also increases the risk of osteoporosis and impedes healing. Coughing due to heavy smoking also may cause back pain.
CAM Therapy for Low Back Pain
CAM Therapy for Low Back Pain
Whiplash
What is Whiplash?
Whiplash-a soft tissue injury to the neck-is also called neck sprain or neck strain. It is characterized by a collection of symptoms that occur following damage to the neck, usually because of sudden extension and flexion. The disorder commonly occurs as the result of an automobile accident and may include injury to intervertebral joints, discs, and ligaments, cervical muscles, and nerve roots. Symptoms such as neck pain may be present directly after the injury or may be delayed for several days. In addition to neck pain, other symptoms may include neck stiffness, injuries to the muscles and ligaments (myofascial injuries), headache, dizziness, abnormal sensations such as burning or prickling (paresthesias), or shoulder or back pain. In addition, some people experience cognitive, somatic, or psychological conditions such as memory loss, concentration impairment, nervousness/irritability, sleep disturbances, fatigue, or depression.
Is there any treatment?
Treatment for individuals with whiplash may include pain medications, nonsteroidal anti-inflammatory drugs, antidepressants, muscle relaxants, and a cervical collar (usually worn for 2 to 3 weeks). Range of motion exercises, physical therapy, and cervical traction may also be prescribed. Supplemental heat application may relieve muscle tension.
What is the prognosis?
Generally, prognosis for individuals with whiplash is good. The neck and head pain clears within a few days or weeks. Most patients recover within 3 months after the injury, however, some may continue to have residual neck pain and headaches.
Piriformis Syndrome aka Pinched Nerve
What is Piriformis Syndrome?
Piriformis syndrome is a rare neuromuscular disorder that occurs when the piriformis muscle compresses or irritates the sciatic nerve-the largest nerve in the body. The piriformis muscle is a narrow muscle located in the buttocks. Compression of the sciatic nerve causes pain-frequently described as tingling or numbness-in the buttocks and along the nerve, often down to the leg. The pain may worsen as a result of sitting for a long period of time, climbing stairs, walking, or running.
Is there any treatment?
Generally, treatment for the disorder begins with stretching exercises and massage. Anti-inflammatory drugs may be prescribed. Cessation of running, bicycling, or similar activities may be advised. A corticosteroid injection near where the piriformis muscle and the sciatic nerve meet may provide temporary relief. In some cases, surgery is recommended.
What is the prognosis?
The prognosis for most individuals with piriformis syndrome is good. Once symptoms of the disorder are addressed, individuals can usually resume their normal activities. In some cases, exercise regimens may need to be modified in order to reduce the likelihood of recurrence or worsening.
What is Pinched Nerve?
The term “pinched nerve” is a colloquial term and not a true medical term. It is used to describe one type of damage or injury to a nerve or set of nerves. The injury may result from compression, constriction, or stretching. Symptoms include numbness, “pins and needles” or burning sensations, and pain radiating outward from the injured area. One of the most common examples of a single compressed nerve is the feeling of having a foot or hand “fall asleep.” A “pinched nerve” frequently is associated with pain in the neck or lower back. This type of pain can be caused by inflammation or pressure on the nerve root as it exits the spine. If the pain is severe or lasts a long time, you may need to have further evaluation from your physician. Several problems can lead to similar symptoms of numbness, pain, and tingling in the hands or feet but without pain in the neck or back. These can include peripheral neuropathy, carpal tunnel syndrome, and tennis elbow. The extent of such injuries may vary from minor, temporary damage to a more permanent condition. Early diagnosis is important to prevent further damage or complications. Pinched nerve is a common cause of on-the-job injury.
Is there any treatment?
The most frequently recommended treatment for pinched nerve is rest for the affected area. Nonsteroidal anti-inflammatory drugs (NSAIDs) or corticosteroids may be recommended to help alleviate pain. Physical therapy is often useful, and splints or collars may be used to relieve symptoms. Depending on the cause and severity of the pinched nerve, surgery may be needed.
What is the prognosis?
With treatment, most people recover from pinched nerve. However, in some cases, the damage is irreversible.
Spinal Stenosis
What Is Spinal Stenosis?
Spinal stenosis is a narrowing of spaces in the spine (backbone) that results in pressure on the spinal cord and/or nerve roots. This disorder usually involves the narrowing of one or more of three areas of the spine:
(1) the canal in the center of the column of bones (vertebral or spinal column) through which the spinal cord and nerve roots run,
(2) the canals at the base or roots of nerves branching out from the spinal cord, or
(3) the openings between vertebrae (bones of the spine) through which nerves leave the spine and go to other parts of the body.
The narrowing may involve a small or large area of the spine. Pressure on the lower part of the spinal cord or on nerve roots branching out from that area may give rise to pain or numbness in the legs. Pressure on the upper part of the spinal cord (that is, the neck area) may produce similar symptoms in the shoulders, or even the legs (see figs.1, 2, and 3).



Who Gets Spinal Stenosis?
Who Gets Spinal Stenosis?
This disorder is most common in men and women over 50 years of age. However, it may occur in younger people who are born with a narrowing of the spinal canal or who suffer an injury to the spine.
What Structures of the Spine Are Involved?
What Structures of the Spine Are Involved?
The spine is a column of 26 bones that extend in a line from the base of the skull to the pelvis (see fig. 1). Twenty-four of the bones are called vertebrae. The bones of the spine include 7 cervical vertebrae in the neck; 12 thoracic vertebrae at the back wall of the chest; 5 lumbar vertebrae at the inward curve (small) of the lower back; the sacrum, composed of 5 fused vertebrae between the hip bones; and the coccyx, composed of 3 to 5 fused bones at the lower tip of the vertebral column. The vertebrae link to each other and are cushioned by shock-absorbing disks that lie between them.
The vertebral column provides the main support for the upper body, allowing humans to stand upright or bend and twist, and it protects the spinal cord from injury. Following are structures of the spine most involved in spinal stenosis (see figs.1, 2, 3, and 7).
- Intervertebral disks. Pads of cartilage filled with a gel-like substance that lie between vertebrae and act as shock absorbers.
- Facet joints. Joints located on the back of the main part of the vertebra. They are formed by a portion of one vertebra and the vertebra above it. They connect the vertebrae to each other and permit backward motion.
- Intervertebral foramen (also called neural foramen). An opening between vertebrae through which nerves leave the spine and extend to other parts of the body.
- Lamina. Part of the vertebra at the back portion of the vertebral arch that forms the roof of the canal through which the spinal cord and nerve roots pass.
- Ligaments. Elastic bands of tissue that support the spine by preventing the vertebrae from slipping out of line as the spine moves. A large ligament often involved in spinal stenosis is the ligamentum flavum, which runs as a continuous band from lamina to lamina in the spine.
- Pedicles. Narrow stem-like structures on the vertebrae that form the walls of the front part of the vertebral arch.
- Spinal cord/nerve roots. A major part of the central nervous system that extends from the base of the brain down to the lower back and that is encased by the vertebral column. It consists of nerve cells and bundles of nerves. The cord connects the brain to all parts of the body via 31 pairs of nerves that branch out from the cord and leave the spine between vertebrae.
- Synovium. A thin membrane that produces fluid to lubricate the facet joints, allowing them to move easily.
- Vertebral arch. A circle of bone around the canal through which the spinal cord passes. It is composed of a floor at the back of the vertebra, walls (the pedicles), and a ceiling where two laminae join.
- Cauda equina. A sack of nerve roots that continues from the lumbar region, where the spinal cord ends, and continues down to provide neurologic function to the lower part of the body. It resembles a “horse’s tail” (cauda equina in Latin).
What Causes Spinal Stenosis?
What Causes Spinal Stenosis?
The normal vertebral canal (see fig. 4) provides adequate room for the spinal cord and cauda equina. Narrowing of the canal, which occurs in spinal stenosis, may be inherited or acquired. Some people inherit a small spinal canal (see fig. 5) or have a curvature of the spine (scoliosis) that produces pressure on nerves and soft tissue and compresses or stretches ligaments. In an inherited condition called achondroplasia, defective bone formation results in abnormally short and thickened pedicles that reduce the diameter (distance across) of the spinal canal.
")

Acquired conditions that can cause spinal stenosis are explained in more detail in the sections that follow.
Degenerative Conditions
Spinal stenosis most often results from a gradual, degenerative aging process. Either structural changes or inflammation can begin the process. As people age, the ligaments of the spine may thicken and calcify (harden from deposits of calcium salts). Bones and joints may also enlarge: when surfaces of the bone begin to project out from the body, these projections are called osteophytes (bone spurs).
When the health of one part of the spine fails, it usually places increased stress on other parts of the spine. For example, a herniated (bulging) disk may place pressure on the spinal cord or nerve root (see fig. 6). When a segment of the spine becomes too mobile, the capsules (enclosing membranes) of the facet joints thicken in an effort to stabilize the segment, and bone spurs may occur. This decreases the space (neural foramen) available for nerve roots leaving the spinal cord.

Spondylolisthesis, a condition in which one vertebra slips forward on another, may result from a degenerative condition or an accident, or, very rarely, may be acquired at birth. Poor alignment of the spinal column when a vertebra slips forward onto the one below it can place pressure on the spinal cord or nerve roots at that place.
Aging with secondary changes is the most common cause of spinal stenosis. Two forms of arthritis that may affect the spine are osteoarthritis and rheumatoid arthritis.
- Osteoarthritis. Osteoarthritis is the most common form of arthritis and is more likely to occur in middle-aged and older people. It is a chronic, degenerative process that may involve multiple joints of the body. It wears away the surface cartilage layer of joints, and is often accompanied by overgrowth of bone, formation of bone spurs, and impaired function. If the degenerative process of osteoarthritis affects the facet joint(s) and the disk, the condition is sometimes referred to as spondylosis. This condition may be accompanied by disk degeneration, and an enlargement or overgrowth of bone that narrows the central and nerve root canals.
- Rheumatoid Arthritis. Rheumatoid arthritis usually affects people at an earlier age than osteoarthritis does and is associated with inflammation and enlargement of the soft tissues (the synovium) of the joints. Although not a common cause of spinal stenosis, damage to ligaments, bones, and joints that begins as synovitis (inflammation of the synovial membrane which lines the inside of the joint) has a severe and disrupting effect on joint function. The portions of the vertebral column with the greatest mobility (for example, the neck area) are often the ones most affected in people with rheumatoid arthritis.
Other Acquired Conditions
The following conditions that are not related to degenerative disease are causes of acquired spinal stenosis:
- Tumors of the spine are abnormal growths of soft tissue that may affect the spinal canal directly by inflammation or by growth of tissue into the canal. Tissue growth may lead to bone resorption (bone loss due to overactivity of certain bone cells) or displacement of bone.
- Trauma (accidents) may either dislocate the spine and the spinal canal or cause burst fractures that produce fragments of bone that penetrate the canal.
- Paget’s disease of bone is a chronic (long-term) disorder that typically results in enlarged and abnormal bones. Excessive bone breakdown and formation cause thick and fragile bone. As a result, bone pain, arthritis, noticeable bone structure changes, and fractures can occur. The disease can affect any bone of the body, but is often found in the spine. The blood supply that feeds healthy nerve tissue may be diverted to the area of involved bone. Also, structural problems of the involved vertebrae can cause narrowing of the spinal canal, producing a variety of neurological symptoms. Other developmental conditions may also result in spinal stenosis.
- Ossification of the posterior longitudinal ligament occurs when calcium deposits form on the ligament that runs up and down behind the spine and inside the spinal canal (see fig. 7). These deposits turn the fibrous tissue of the ligament into bone. (Ossification means “forming bone.”) These deposits may press on the nerves in the spinal canal.

What Are the Symptoms of Spinal Stenosis?
What Are the Symptoms of Spinal Stenosis?
The space within the spinal canal may narrow without producing any symptoms. However, if narrowing places pressure on the spinal cord, cauda equina, or nerve roots, there may be a slow onset and progression of symptoms. The neck or back may or may not hurt. More often, people experience numbness, weakness, cramping, or general pain in the arms or legs. If the narrowed space within the spine is pushing on a nerve root, people may feel pain radiating down the leg (sciatica). Sitting or flexing the lower back should relieve symptoms. (The flexed position “opens up” the spinal column, enlarging the spaces between vertebrae at the back of the spine.) Flexing exercises are often advised, along with stretching and strengthening exercises.
People with more severe stenosis may have problems with bowel and bladder function and foot disorders. For example, cauda equina syndrome is a severe, and very rare, form of spinal stenosis. It occurs because of compression of the cauda equina, and symptoms may include loss of control of the bowel, bladder, or sexual function and/or pain, weakness, or loss of feeling in one or both legs. Cauda equina syndrome is a serious condition requiring urgent medical attention.
How Is Spinal Stenosis Diagnosed?
How Is Spinal Stenosis Diagnosed?
The doctor may use a variety of approaches to diagnose spinal stenosis and rule out other conditions.
- Medical history. The patient tells the doctor details about symptoms and about any injury, condition, or general health problem that might be causing the symptoms.
- Physical examination. The doctor (1) examines the patient to determine the extent of limitation of movement, (2) checks for pain or symptoms when the patient hyper-extends the spine (bends backwards), and (3) checks for normal neurologic function (for instance, sensation, muscle strength, and reflexes) in the arms and legs.
- X ray. An x-ray beam is passed through the back to produce a two-dimensional picture. An x ray may be done before other tests to look for signs of an injury, tumor, or inherited problem. This test can show the structure of the vertebrae and the outlines of joints, and can detect calcification.
- MRI magnetic resonance imaging). Energy from a powerful magnet (rather than x rays) produces signals that are detected by a scanner and analyzed by computer. This produces a series of cross-sectional images (“slices”) and/or a three-dimensional view of parts of the back. An MRI is particularly sensitive for detecting damage or disease of soft tissues, such as the disks between vertebrae or ligaments. It shows the spinal cord, nerve roots, and surrounding spaces, as well as enlargement, degeneration, or tumors.
- Computerized axial tomography (CAT). X rays are passed through the back at different angles, detected by a scanner, and analyzed by a computer. This produces a series of cross-sectional images and/or three-dimensional views of the parts of the back. The scan shows the shape and size of the spinal canal, its contents, and structures surrounding it.
- Myelogram. A liquid dye that x rays cannot penetrate is injected into the spinal column. The dye circulates around the spinal cord and spinal nerves, which appear as white objects against bone on an x-ray film. A myelogram can show pressure on the spinal cord or nerves from herniated disks, bone spurs, or tumors.
- Bone scan. An injected radioactive material attaches itself to bone, especially in areas where bone is actively breaking down or being formed. The test can detect fractures, tumors, infections, and arthritis, but may not tell one disorder from another. Therefore, a bone scan is usually performed along with other tests.
Who Treats Spinal Stenosis?
Who Treats Spinal Stenosis?
Nonsurgical treatment of spinal stenosis may be provided by internists or general practitioners. The disorder is also treated by specialists such as rheumatologists, who treat arthritis and related disorders; and neurologists, who treat nerve diseases. Orthopaedic surgeons and neurosurgeons also provide nonsurgical treatment and perform spinal surgery if it is required. Allied health professionals such as physical therapists may also help treat patients.
What Are Some Nonsurgical Treatments for Spinal Stenosis?
What Are Some Nonsurgical Treatments for Spinal Stenosis?
In the absence of severe or progressive nerve involvement, a doctor may prescribe one or more of the following conservative treatments:
- Nonsteroidal anti–inflammatory drugs (NSAIDs), such as aspirin, naproxen, ibuprofen, or indomethacin, to reduce inflammation and relieve pain.1
- Analgesics, such as acetaminophen, to relieve pain.
- Corticosteroid injections into the outermost of the membranes covering the spinal cord and nerve roots to reduce inflammation and treat acute pain that radiates to the hips or down a leg.
- Anesthetic injections, known as nerve blocks, near the affected nerve to temporarily relieve pain.
- Restricted activity (varies depending on extent of nerve involvement).
- Prescribed exercises and/or physical therapy to maintain motion of the spine, strengthen abdominal and back muscles, and build endurance, all of which help stabilize the spine. Some patients may be encouraged to try slowly progressive aerobic activity such as swimming or using exercise bicycles.
- A lumbar brace or corset to provide some support and help the patient regain mobility. This approach is sometimes used for patients with weak abdominal muscles or older patients with degeneration at several levels of the spine.
1 Warning: Side effects of NSAIDs include stomach problems; skin rashes; high blood pressure; fluid retention; and liver, kidney, and heart problems. The longer a person uses NSAIDs, the more likely he or she is to have side effects, ranging from mild to serious. Many other drugs cannot be taken when a patient is being treated with NSAIDs, because NSAIDs alter the way the body uses or eliminates these other drugs. Check with your health care provider or pharmacist before you take NSAIDs. NSAIDs should only be used at the lowest dose possible for the shortest time needed.
What Are Some Alternative Therapies for Spinal Stenosis?
What Are Some Alternative Therapies for Spinal Stenosis?
Alternative (or complementary) therapies are diverse medical and health care systems, practices, and products that are not presently considered to be part of conventional medicine. Some examples of these therapies used to treat spinal stenosis follow:
- Chiropractic treatment. This treatment is based on the philosophy that restricted movement in the spine reduces proper function and may cause pain. Chiropractors may manipulate (adjust) the spine to restore normal spinal movement. They may also employ traction, a pulling force, to help increase space between the vertebrae and reduce pressure on affected nerves. Some people report that they benefit from chiropractic care. Research thus far has shown that chiropractic treatment is about as effective as conventional, nonoperative treatments for acute back pain.
- Acupuncture. This treatment involves stimulating certain places on the skin by a variety of techniques, in most cases by manipulating thin, solid, metallic needles that penetrate the skin. Research has shown that low back pain is one area in which acupuncture has benefited some people.
More research is needed before the effectiveness of these or other possible alternative therapies can be definitively stated. Health care providers may suggest these therapies in addition to more conventional treatments.
When Should Surgery Be Considered and What Is Involved?
When Should Surgery Be Considered and What Is Involved?
In many cases, the conditions causing spinal stenosis cannot be permanently altered by nonsurgical treatment, even though these measures may relieve pain for a period of time. To determine how much nonsurgical treatment will help, a doctor may recommend such treatment first. However, surgery might be considered immediately if a patient has numbness or weakness that interferes with walking, impaired bowel or bladder function, or other neurological involvement. The effectiveness of nonsurgical treatments, the extent of the patient’s pain, and the patient’s preferences may all factor into whether or not to have surgery.
The purpose of surgery is to relieve pressure on the spinal cord or nerves and restore and maintain alignment and strength of the spine. This can be done by removing, trimming, or adjusting diseased parts that are causing the pressure or loss of alignment. The most common surgery is called decompressive laminectomy: removal of the lamina (roof) of one or more vertebrae to create more space for the nerves. A surgeon may perform a laminectomy with or without fusing vertebrae or removing part of a disk. Various devices may be used to enhance fusion and strengthen unstable segments of the spine following decompression surgery.
Patients with spinal stenosis caused by spinal trauma or achondroplasia may need surgery at a young age. When surgery is required in patients with achondroplasia, laminectomy (removal of the roof) without fusion is usually sufficient.
What Are the Major Risks of Surgery?
What Are the Major Risks of Surgery?
All surgery, particularly that involving general anesthesia and older patients, carries risks. The most common complications of surgery for spinal stenosis are a tear in the membrane covering the spinal cord at the site of the operation, infection, or a blood clot that forms in the veins. These conditions can be treated but may prolong recovery. The presence of other diseases and the physical condition of the patient are also significant factors to consider when making decisions about surgery.
What Are the Long-Term Outcomes of Surgical Treatment for Spinal Stenosis?
What Are the Long-Term Outcomes of Surgical Treatment for Spinal Stenosis?
Removal of the obstruction that has caused the symptoms usually gives patients some relief; most patients have less leg pain and are able to walk better following surgery. However, if nerves were badly damaged before surgery, there may be some remaining pain or numbness or no improvement. Also, the degenerative process will likely continue, and pain or limitation of activity may reappear after surgery. NIAMS-supported researchers have published results from the Spine Patient Outcomes Research Trial (SPORT), the largest trial to date comparing surgical and non-surgical interventions for the treatment of low back and associated leg pain caused by spinal stenosis. The study found that for patients with spinal stenosis, surgical treatment was more effective than non-surgical treatment in relieving symptoms and improving function. However, the functional status of patients who received non-surgical therapies also improved somewhat during the study.
Attribution
1. National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS.NIH.gov)
2. National Institutes of Health (NIH.gov)

Back Pain Condition brochures
Degenerative Disc Disease
Facet Joint Syndrome
Herniated Discs
Myofascial Pain Syndrome
Post-Laminectomy Syndrome
Spinal Stenosis
Back Pain Treatment brochures
Facet Joint Injections
Lumbar Epidural Steroid Injection
Lumbar Sympathetic Block
Lumbar Transforaminal Epidural Steroid Injection
Medial Branch Block
Radiofrequency Neurotomy of the Lumbar Facets
Sacroiliac Joint Steroid Injection
Spinal Cord Stimulator Implant (Trial Procedure)
Stellate Ganglion Block
Degenerative Disc Disease
Facet Joint Syndrome
Herniated Discs
Myofascial Pain Syndrome
Post-Laminectomy Syndrome
Spinal Stenosis

Facet Joint Injections
Lumbar Epidural Steroid Injection
Lumbar Sympathetic Block
Lumbar Transforaminal Epidural Steroid Injection
Medial Branch Block
Radiofrequency Neurotomy of the Lumbar Facets
Sacroiliac Joint Steroid Injection
Spinal Cord Stimulator Implant (Trial Procedure)
Stellate Ganglion Block

Boston Scientific: Precision Spectra™ Spinal Cord Stimulator System
The Boston Scientific Precision Spectra™ Spinal Cord Stimulator (SCS) System provides more pain relief to a broader spectrum of patients – watch the 26 second video below for an overview on how SCS works:
Additional SCS Information direct from the Boston Scientific website:
SCS - Real Patient Stories
The Boston Scientific SCS system works to interrupt pain impulses before they reach the brain to help patients manage their pain • Some patients say SCS feels like a gentle fluttering sensation that replaces the pain • The term some would choose is “relief”
Scroll through the window frame below to Watch the 10 Patient Testimonial Videos – hear directly from Real Boston Scientific Spinal Cord Stimulation (SCS) Patients:
